Table of Contents
- What Are the Similarities and Differences Between Schizoid and Schizotypal Personality Disorders?
- Diagnostic Criteria: DSM-5 Perspective
- Presentation in Therapy: Recognizing the Differences
- Case Study: Differentiating SPD and STPD in Clinical Practice
- Treatment Approaches: Tailoring Interventions
- Enhancing Your Clinical Skills with Continuing Education
- Conclusion
- References
As mental health professionals, we often encounter complex cases that challenge our diagnostic skills and treatment approaches. Two conditions that frequently cause confusion due to their similarities are schizoid personality disorder (SPD) and schizotypal personality disorder (STPD). This comprehensive guide will explore the key differences and similarities between these disorders, providing you with valuable insights to enhance your clinical practice.
What Are the Similarities and Differences Between Schizoid and Schizotypal Personality Disorders?
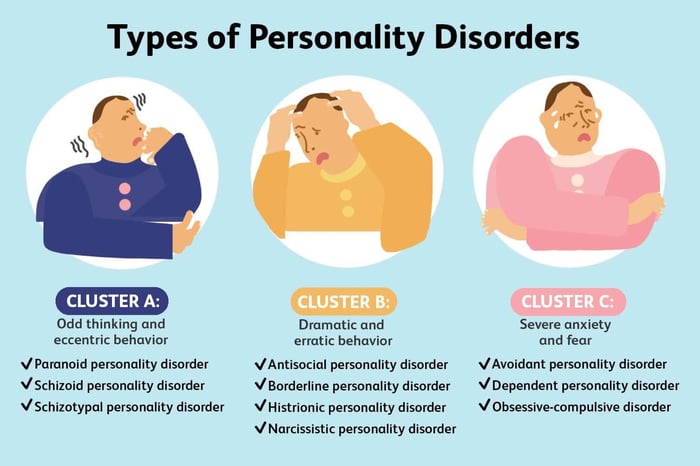
Both schizoid and schizotypal personality disorders fall within the Cluster A personality disorders, often referred to as "odd or eccentric" disorders. While they share some common features, such as social withdrawal and difficulties in interpersonal relationships, there are crucial distinctions that set them apart.
Schizoid Personality Disorder (SPD)
Schizoid personality disorder is characterized by a pervasive pattern of detachment from social relationships and a restricted range of emotional expression. Individuals with SPD often appear aloof, indifferent to social interactions, and prefer solitary activities.
Key features of SPD include:
- Limited interest in social relationships
- Emotional coldness or flattened affect
- Little to no desire for sexual experiences
- Indifference to praise or criticism
- Limited capacity for pleasure
Schizotypal Personality Disorder (STPD)
Schizotypal personality disorder is marked by acute discomfort in close relationships, cognitive or perceptual distortions, and eccentricities of behavior. People with STPD often have odd beliefs or magical thinking that influences their behavior.
Key features of STPD include:
- Ideas of reference (incorrect interpretation of casual incidents as having personal meaning)
- Odd beliefs or magical thinking
- Unusual perceptual experiences
- Odd thinking and speech
- Paranoid ideation
- Inappropriate or constricted affect
- Odd behavior or appearance
- Lack of close friends or confidants
Diagnostic Criteria: DSM-5 Perspective
To accurately diagnose these disorders, it's essential to understand the specific criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).
Schizoid Personality Disorder Criteria
A pervasive pattern of detachment from social relationships and a restricted range of expression of emotions in interpersonal settings, beginning by early adulthood and present in a variety of contexts, as indicated by four (or more) of the following:
- Neither desires nor enjoys close relationships, including being part of a family
- Almost always chooses solitary activities
- Has little, if any, interest in having sexual experiences with another person
- Takes pleasure in few, if any, activities
- Lacks close friends or confidants other than first-degree relatives
- Appears indifferent to the praise or criticism of others
- Shows emotional coldness, detachment, or flattened affectivity
Schizotypal Personality Disorder Criteria
A pervasive pattern of social and interpersonal deficits marked by acute discomfort with, and reduced capacity for, close relationships as well as by cognitive or perceptual distortions and eccentricities of behavior, beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following:
- Ideas of reference (excluding delusions of reference)
- Odd beliefs or magical thinking that influences behavior and is inconsistent with subcultural norms
- Unusual perceptual experiences, including bodily illusions
- Odd thinking and speech
- Suspiciousness or paranoid ideation
- Inappropriate or constricted affect
- Behavior or appearance that is odd, eccentric, or peculiar
- Lack of close friends or confidants other than first-degree relatives
- Excessive social anxiety that does not diminish with familiarity and tends to be associated with paranoid fears rather than negative judgments about self
Presentation in Therapy: Recognizing the Differences
When working with clients who may have either SPD or STPD, it's crucial to observe their behavior and communication style during therapy sessions. Here are some key differences you might notice:
Schizoid Personality Disorder
- Clients with SPD may appear emotionally distant and uninterested in forming a therapeutic alliance.
- They might struggle to express emotions or discuss personal matters.
- These individuals often report a preference for solitary activities and may resist efforts to explore interpersonal relationships.
Schizotypal Personality Disorder
- Clients with STPD may exhibit odd or eccentric behavior during sessions.
- They might express unusual beliefs or describe strange perceptual experiences.
- These individuals may be more overtly anxious or paranoid compared to those with SPD.
- Their speech patterns might be peculiar, with tangential or circumstantial communication.
Case Study: Differentiating SPD and STPD in Clinical Practice
To illustrate the differences between these disorders, let's consider the following case study:
Case Presentation:Sarah, a 32-year-old software developer, was referred for therapy by her employer due to concerns about her work performance and interactions with colleagues. During the initial assessment, you observe the following:
- Sarah appears uncomfortable and avoids eye contact.
- She speaks in a monotone voice and provides minimal elaboration on her responses.
- When asked about her social life, Sarah states that she prefers to be alone and has no close friends.
- She mentions that she sometimes feels that her computer is sending her secret messages through code patterns.
- Sarah describes a belief that she can influence the weather with her thoughts.
Discussion:While Sarah exhibits some features common to both SPD and STPD, her presentation more closely aligns with schizotypal personality disorder. The key differentiating factors include:
- Presence of odd beliefs and magical thinking (influencing weather with thoughts)
- Ideas of reference (secret messages through code patterns)
- Social anxiety with paranoid features (uncomfortable in the session)
These features are more characteristic of STPD than SPD. A person with SPD would be less likely to express such unusual beliefs or perceptual experiences.
Treatment Approaches: Tailoring Interventions
Effective treatment for both disorders typically involves psychotherapy, with potential pharmacological interventions for specific symptoms. However, the approach may differ based on the specific disorder and individual needs.
Schizoid Personality Disorder Treatment
- Focus on gradually building the therapeutic relationship, respecting the client's need for emotional distance
- Explore and validate the client's inner emotional world
- Cognitive-behavioral techniques to address maladaptive thoughts about relationships
- Support in developing social skills, if the client expresses interest
Schizotypal Personality Disorder Treatment
- Cognitive-behavioral therapy to address distorted thinking patterns and social anxiety
- Social skills training to improve interpersonal functioning
- Supportive therapy to provide a stable, non-threatening environment
- Possible use of low-dose antipsychotic medications for perceptual disturbances or paranoid symptoms
Enhancing Your Clinical Skills with Continuing Education
As mental health professionals, staying updated with the latest research and treatment modalities is crucial for providing the best care to our clients. Therapy Trainings™ offers a wide range of continuing education courses specifically designed for mental health professionals looking to deepen their understanding of complex personality disorders.
Our courses, available at therapytrainings.com, are approved by licensing boards across the nation, ensuring that you can earn CE credits while enhancing your clinical skills. Whether you're looking to refine your diagnostic abilities or explore innovative treatment approaches for personality disorders, our expert-led training programs can help you stay at the forefront of mental health care.
Conclusion
Understanding the nuances between schizoid and schizotypal personality disorders is essential for accurate diagnosis and effective treatment planning. By recognizing the distinct features of each disorder, mental health professionals can provide more targeted and compassionate care to individuals struggling with these complex conditions.
Knowledge of the two is essential for distinguishing between these closely related disorders, and to complement this, try reading our blog Reliability vs. Validity in Psychological Assessment: A Comprehensive Guide for Mental Health Professionals can ensure that the diagnostic tools used are both accurate and dependable, leading to more precise assessments and effective treatment planning.
Continue your professional development journey with Therapy Trainings™ and explore our comprehensive CE courses on personality disorders and other critical topics in mental health. Visit therapytrainings.com today to discover how you can enhance your clinical practice and make a lasting impact on your clients' lives.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
- Kirchner, S. K., Roeh, A., Nolden, J., & Hasan, A. (2018). Diagnosis and treatment of schizotypal personality disorder: evidence from a systematic review. NPJ Schizophrenia, 4(1), 20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6220141/
- Martens, W. H. (2010). Schizoid personality disorder linked to unbearable and inescapable loneliness. The European Journal of Psychiatry, 24(1), 38-45. https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-61632010000100005
- Rosell, D. R., Futterman, S. E., McMaster, A., & Siever, L. J. (2014). Schizotypal personality disorder: a current review. Current Psychiatry Reports, 16(7), 452.
- Triebwasser, J., Chemerinski, E., Roussos, P., & Siever, L. J. (2012). Schizoid personality disorder. Journal of Personality Disorders, 26(6), 919-926.



