Table of Contents
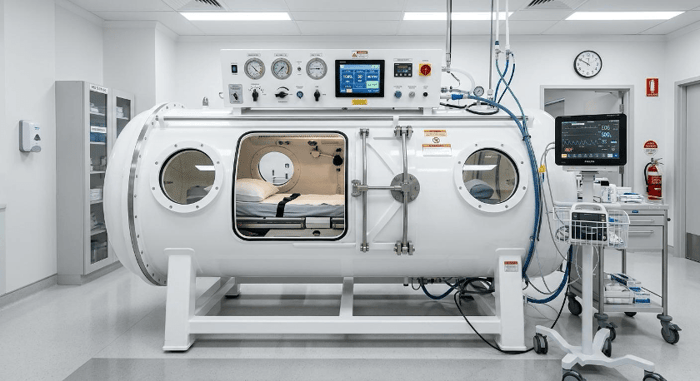 A clinical-grade hyperbaric oxygen chamber - the kind used in psychiatric research trials, distinct from the soft-shell consumer versions many clients encounter first.
A clinical-grade hyperbaric oxygen chamber - the kind used in psychiatric research trials, distinct from the soft-shell consumer versions many clients encounter first.
It’s happening more often. A client mentions they’ve been researching hyperbaric oxygen therapy. Maybe they read about it in a veteran’s community forum, or a friend with treatment-resistant PTSD swears by it. They want to know what you think.
If your continuing education hasn’t covered HBOT yet, you’re not alone - the research has moved faster than most clinical training programs have caught up. But the 2024-2025 data is rigorous enough that therapeutic unfamiliarity is becoming a real gap, especially for clinicians who regularly work with PTSD, traumatic brain injury, or treatment-resistant presentations.
This isn’t a consumer overview. It’s a clinical briefing. What follows covers the biological mechanism, the strongest evidence currently available, where that evidence has limits, and what you need to know before clients ask - because they will.
How HBOT Works: The Basics Every Clinician Should Understand
A hyperbaric oxygen chamber pressurizes air to 1.5 to 2.0 atmospheres absolute (ATA) while the patient breathes 100% oxygen. Under normal atmospheric pressure, oxygen binds almost entirely to hemoglobin. Under hyperbaric conditions, oxygen dissolves directly into blood plasma - bypassing the hemoglobin pathway entirely. This pushes oxygen concentrations in tissue well above what normal breathing can achieve.
For the brain, that distinction matters more than it might seem. The brain consumes roughly 20% of the body’s total oxygen while accounting for just 2% of body weight. Injured or chronically hypoxic brain tissue - the kind commonly found in PTSD and TBI - is particularly responsive to elevated oxygen delivery.
What makes HBOT’s neurological effects more than simple oxygen flooding is something researchers call the hyperoxic-hypoxic paradox. Repeated cycles of elevated then normalized oxygen are perceived by cells as brief hypoxia. The body’s stress response kicks in - specifically the upregulation of hypoxia-inducible factor (HIF) - which triggers a cascade of cellular repair processes: mitochondrial biogenesis, neurogenesis, synaptogenesis, and anti-inflammatory signaling. A 2024 review in PMC summarized this mechanism as a form of physiological hormesis, in which controlled oxygen stress induces measurable adaptive repair at the cellular level.
The FDA has approved HBOT for 13 conditions, including decompression sickness, carbon monoxide poisoning, and chronic wound healing. All psychiatric applications are currently off-label - a distinction that matters when you’re advising clients on what to expect from medical providers.
One thing your clients will encounter before they ever visit a clinic: a consumer market. People researching HBOT on their own will find hyperbaric oxygen therapy chambers for sale across a wide range of pressure specifications. Soft-shell consumer chambers typically operate at 1.3 ATA - below the 1.5 to 2.0 ATA threshold used in the psychiatric trials discussed below. That gap is clinically significant, and it’s a practical point worth raising when clients ask whether they can replicate a clinical protocol at home.
The PTSD Evidence: What Clinical Trials Actually Show
fMRI data from the 2024 Journal of Clinical Psychiatry HBOT trial show measurable increases in connectivity within brain networks governing emotional regulation, memory, and executive function.
For therapists who treat trauma, this is the most relevant section. The evidence for HBOT in PTSD is not preliminary - it’s among the strongest data on any off-label neurological intervention in the current literature.
A 2024 randomized, sham-controlled trial published in the Journal of Clinical Psychiatry enrolled combat veterans with treatment-resistant PTSD - defined as having failed at least one full course each of trauma-focused psychotherapy and pharmacotherapy. After 60 HBOT sessions over three months, 68% of the treatment group showed at least 30% reduction in PTSD symptom severity, compared to 4% in the sham group. Full remission was achieved by 39% of HBOT participants, compared with 0% in controls. fMRI data confirmed what symptom scores suggested - significantly increased connectivity in the frontoparietal network, default mode network, and between the right dorsolateral prefrontal cortex and the thalamus.
That’s not a subtle result. For clients who’ve cycled through CPT, EMDR, and multiple medication trials without adequate relief, these numbers represent a genuinely different order of magnitude from what’s typically seen in treatment-resistant populations.
A 2024 systematic review in Frontiers in Neurology analyzed 8 studies covering 393 subjects. All 7 RCTs scored between 7 and 9 on the PEDro methodological quality scale. The review confirmed a dose-response relationship - more sessions produced better outcomes - and found that benefits generalized across military and civilian populations, both sexes, and multiple trauma types, including combat and sexual trauma.
A 2025 post hoc analysis by researchers at the Weizmann Institute and the Sagol Center for Hyperbaric Medicine identified what they termed a threshold effect: veterans who achieved at least 35% symptom improvement by the end of treatment maintained those gains at the 3-month follow-up (p = 2e-6). Those who didn’t reach that threshold showed attenuation. Avoidance symptoms - Cluster C on the PTSD Checklist - were the strongest predictor of durable gains (r = 0.70). This suggests HBOT may be doing something neuroplastic, not just symptomatic.
There’s a clinical nuance you should know before any client starts a high-dose protocol. Between 30 and 39% of subjects in intensive HBOT trials experienced a temporary exacerbation of emotional symptoms - memory surfacing, increased distress. These effects were reversible and manageable, but your clients may need additional support during treatment. Plan for that proactively.
The bottom line, stated plainly: HBOT doesn’t replace evidence-based treatment for PTSD. What it may do is restore the neurobiological conditions that allow those treatments to work. For clients who’ve hit the ceiling of first-line interventions, that’s a meaningful distinction.
TBI, Cognitive Impairment, and the Mental Health Overlap

A 2025 Neurology meta-analysis found significant improvements in memory, attention, and executive function in TBI patients following HBOT, suggesting that neuroplastic recovery is possible even in chronic cases.
The numbers from the Department of Defense are hard to sit with. According to the DoD TBI Center of Excellence, 514,583 U.S. service members have been affected by TBI since 2000. Among OEF/OIF veterans with TBI receiving VA services, 89% had a co-occurring psychiatric diagnosis, and PTSD was the most common, affecting 73% of that group.
What therapists see in practice is the cascade. TBI disrupts working memory, processing speed, and executive function. Those disruptions lead to frustration, avoidance, social withdrawal, and depressive symptoms. The depressive symptoms then compound the cognitive deficits. Clients come in with presentations that look like several overlapping conditions because, in many cases, there are several overlapping conditions.
An April 2025 meta-analysis in Neurology - the most recent and methodologically rigorous analysis in this area - found HBOT significantly improved neurocognitive deficits in TBI patients compared to baseline across multiple domains: general cognitive scores (MD 7.47, p=0.003), memory (MD 10.13, p<0.00001), attention (MD 7.99, p<0.00001), and executive function (MD 7.16, p=0.002). These aren’t marginal shifts. Memory improvements at that effect size are clinically detectable and reportable by patients.
A separate 2025 Frontiers in Neurology retrospective cohort study found something that will matter to many of your clients: adults who had experienced TBI as children and were still symptomatic in adulthood - post-concussion syndrome in the late chronic phase, sometimes years after the original injury - showed measurable improvement under HBOT. The implication is that neuroplastic recovery doesn’t require recency. That’s worth knowing when clients who’ve been symptomatic for a decade tell you they assume they’ve hit their ceiling.
On dosing: the evidence suggests there’s a useful range and that exceeding it doesn’t add benefit. Some research on moderate TBI points to an optimal window of around 40 to 60 sessions at 2.0 ATA. The HBOT protocols that produced the strongest psychiatric outcomes in TBI were individualized and medically supervised - not consumer protocols.
Depression and Anxiety: A More Cautious Picture
The evidence gradient here is real, and you should describe it honestly to clients who ask.
For PTSD and TBI-related conditions, the clinical trial data are rigorous, and the effect sizes are large. For primary depression or anxiety without any underlying neurological history, the data is more preliminary and shouldn’t be represented to clients as established.
The biological pathway is credible. Mitochondrial dysfunction is a documented contributor to major depressive disorder. When neurons can’t produce sufficient ATP, the downstream effects include mood dysregulation, cognitive slowing, and fatigue. Oxygen-based interventions directly address mitochondrial function, which provides HBOT with a plausible mechanism for mood applications.
The most frequently cited mood data in this space comes from a Ben-Gurion University study reporting 69% improvement in depression scores versus 23% in controls. That study used normobaric oxygen rather than hyperbaric oxygen - the plasma-dissolving mechanism that distinguishes HBOT wasn’t fully in play. fMRI data from HBOT trials show improvements in hippocampal and insular cortex activation, both implicated in emotional regulation and threat detection.
That said, for a client presenting with major depressive disorder and no history of TBI, stroke, or post-COVID neurological symptoms, HBOT is not a clinically validated adjunct. Don’t frame it as one. The responsible position right now is to watch the research - larger RCTs for primary mood disorders are underway - and update your framing as the data matures.
For clients with depression in the context of TBI, stroke, or long COVID-related cognitive symptoms, the biological case for discussing HBOT is much stronger. That’s where referral conversations become appropriate.
What Clinicians Should Know Before the Conversation Happens

As HBOT research gains clinical traction, therapists are increasingly the first professional clients turn to with questions - making familiarity with the evidence an important part of informed care.
When a client brings up HBOT, they’re usually not asking you to prescribe it. They’re asking you to help them think through it. Here’s what you need for that conversation.
The psychiatric protocols studied in clinical trials run 40 to 60 sessions, typically 60 to 90 minutes each, at 1.5 to 2.0 ATA. In clinical settings, sessions cost between $150 and $650 each. That’s a significant access barrier, and it’s one that clients often haven’t fully accounted for when they bring it up. At-home soft-shell options cost less but operate at pressure levels below those used in the trials - a difference clients deserve to understand before investing.
All psychiatric applications of HBOT are currently off-label. The FDA hasn’t approved it for PTSD, depression, TBI-related psychiatric symptoms, or any other mental health condition. That doesn’t mean the evidence is weak - the clinical trial data reviewed above is substantial. But it does mean clients won’t have the same insurance coverage and informed-consent protections they’d have with a first-line treatment.
The clients most likely to benefit from a referral conversation are those with treatment-resistant PTSD who’ve failed at least one course of trauma-focused therapy and pharmacotherapy, those with TBI-related persistent psychiatric symptoms, and those with post-COVID cognitive and mood complaints. Clients with MRI-confirmed brain changes may also be appropriate candidates, depending on the clinical picture.
Contraindications include untreated claustrophobia, untreated pneumothorax, recent ear or sinus surgery, and certain cardiac conditions. Any client pursuing HBOT will need a full medical evaluation before starting - that’s standard protocol at reputable facilities.
The risk of temporary emotional exacerbation is the most important clinical consideration for therapists. Up to 39% of participants in high-dose HBOT trials experienced temporary intensification of symptoms during treatment - increased distress, intrusive memories surfacing. It’s reversible. But your clients may need more frequent contact during a course of treatment, and they should know this is possible before they start. Framing HBOT as an adjunct to the existing therapeutic relationship - not a detour from it - is both accurate to the research and good clinical practice.
For practices that work with multidisciplinary teams, understanding types of therapists and their roles in a collaborative care model matters here: HBOT decisions are best made with a medical provider involved, and the therapist’s role is informed support and coordination rather than recommendation or prescription.
Conclusion
The 2024-2025 research on HBOT and mental health isn’t speculative. For treatment-resistant PTSD and TBI-related cognitive and psychiatric symptoms, the evidence is rigorous, the effect sizes are real, and the biological mechanisms are well-characterized. That doesn’t make HBOT a first-line treatment - it isn’t one, and it shouldn’t be framed that way. But it does mean that clinical unfamiliarity with this intervention is becoming a professional gap.
HBOT won’t replace psychotherapy. For clients who’ve already done the work in therapy and haven’t responded adequately, it may restore the neurological conditions that make psychotherapy work. That’s a different kind of tool from the one therapists are used to thinking about, and it’s worth understanding.
Staying current on emerging, evidence-backed adjuncts - knowing what the trials show, where the evidence is strong, where it’s preliminary, and what clients should realistically expect - is part of competent, client-centered practice. The field is moving. Clients are researching independently and making decisions with or without clinical guidance. Being the informed professional they turn to first is a better position than being the one who has to catch up after they’ve already started.